{kind=link}
The clavicle fracture (broken collarbone), is one of the most common acute shoulder and are quite common in sport which actually account for 2-5% of all adult fractures and seeing even more fractures in adolescents.
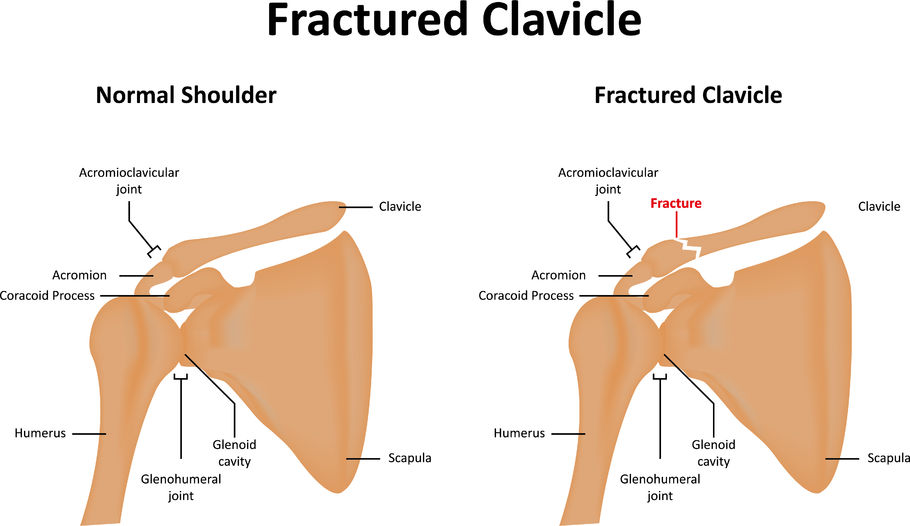
The clavicle is a long bone in the body that is located between the ribcage and the shoulder blade; it is most commonly broken at the middle third or known as mid-shaft where it is weakest.
Clavicle fractures are often caused by a direct blow to the shoulder, which can happen during a collision, direct impact, or falling on an out stretched hand (FOOSH). In athlete’s, these types of injuries can be quite common due to the mechanisms in which athletes get hit or fall in contact sports as you most likely saw Tony Romo fall on an outstretched arm this past week.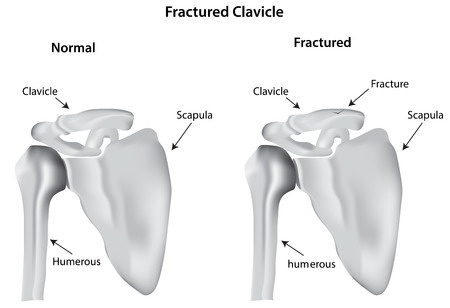
Clavicle fractures can be very painful and may make it hard for one to move their arm. Additional symptoms include:
- Sagging shoulder (down and forward)
- Inability to lift the arm because of pain
- A grinding sensation if an attempt is made to raise the arm
- A deformity or “bump” over the break site
- Bruising, swelling, and/or tenderness over the collarbone
Treatment for any broke bone includes restricting movement or immobilize to allow healing. To immobilize a broken clavicle, wearing an armsling for 6-12 weeks is typical. Rehabilitation or Physical Therapy is also recommended after the sling is removed to restore joint mobility, flexibility, and muscular and functional strength.
Sometimes surgery is required depending on the severity, whether it’s displaced or a compound fracture (broken through the skin).
Can an athlete come back after a broken collarbone? Of course! However their recovery timeline always varies depending on level of play, sport, rehabilitation, and how the specific athletes body heals.
Jessica Thomas MS, ATC, CHC